.  |
I received my Masters in Social Work from Michigan State University in 1971 and was a psychotherapist until my retirement. My main salaried work experience was with one of the best community mental health programs in the country, Clinton-Eaton-Ingham Community Mental Health Board headquartered in Lansing, Michigan. I always had a private practice along with my salaried job.
RIP:

My friend and colleague Mel was one of the original Three Musketeers as we sometimes called ourselves, the first staff therapists who worked together when the Mason Mental Health Center opened, died in 2022. Mel and I worked closely together along with Mary Louis, MSW to literally build Mason Mental Health Center by constructing walls to make offices out of large rooms in our building and of course we put together a program serving the previously poorly served small town and rural areas of the Ingham County where most of Lansing is located.
As newly credentialed therapists we made up in enthusiasm and caring for our clients what we lacked in experience. We provided clinical supervision to each other and with nobody to tell us not to try new approaches we learned and grew as therapists from our successes and thankfully very few failures.
Much credit is due to the program's supervisor, the late Ben Perri, PhD who didn't have much more clinical experience than we did, for having the wisdom to hire the three of us and allowing us the freedom to learn and grow.
In those early days we didn't have time limits for how long we could see clients and when appropriate could we could see them more than once a week or partner with another therapist and do co-therapy. We weren't held back by the rules of insurance companies or Medicare and of having to use check-lists that pigeon-holed clients into a set of problems and our setting observable goals. We just treated our clients as we'd want to be treated ourselves: as real people with real feelings.
The rules were relaxed in another important way at that time. I had much more leeway in who I hired and promoted. For example Marilyn Braman was our van driver and Jackie Lawrence was one of our secretaries. Neither had college degrees but both demonstrated such rapport with clients that when I had an opening in the day treatment program I promoted them to be mental health workers, basically aides who did pretty much the same thing the credentialed staff. I hired Jim Mueller as a therapist in day treatment even though his BA was in philosophy. He went on to get his MSW at Smith College which has the best clinical social work program in the country. Notably I hired Linda Ward who had a BSW to design and run the day treatment and aftercare programs. A year or two later that job would have required at least a masters degree. She put together a program that turned out to be a model program emulated by other programs around the state.
We also saw many outpatient clients for a token fee of $2.00.
The History of Mason Mental Health Center
by Hal Brown
(click images to enlarge)
The original staff in 1971
Top row: Mel Scherpinesse, MA; Ben Perri, PhD (Director); Hal Brown, MSW
Bottom row: Mary Louis, MSW; Barb Hollenbeck, and Ellen Martinson; our secretaries.


Tom Helma, MA, was the second director
From its inception at the very beginning of the era where public mental health services were generously funded, the Mason Mental Health Center was a barometer of the value government placed on providing high quality outpatient mental health services to people in locations that were easily accessible.
The Mason program itself was a branch office of a much larger program located in Lansing, Michigan. The town of Mason had a population of 5,500, but the rural area it served had a population of over 35,000. We ran clinics in three outlying towns in the corners of the county (Leslie, Stockbridge, and Williamston), and brought our services to an underserved population.
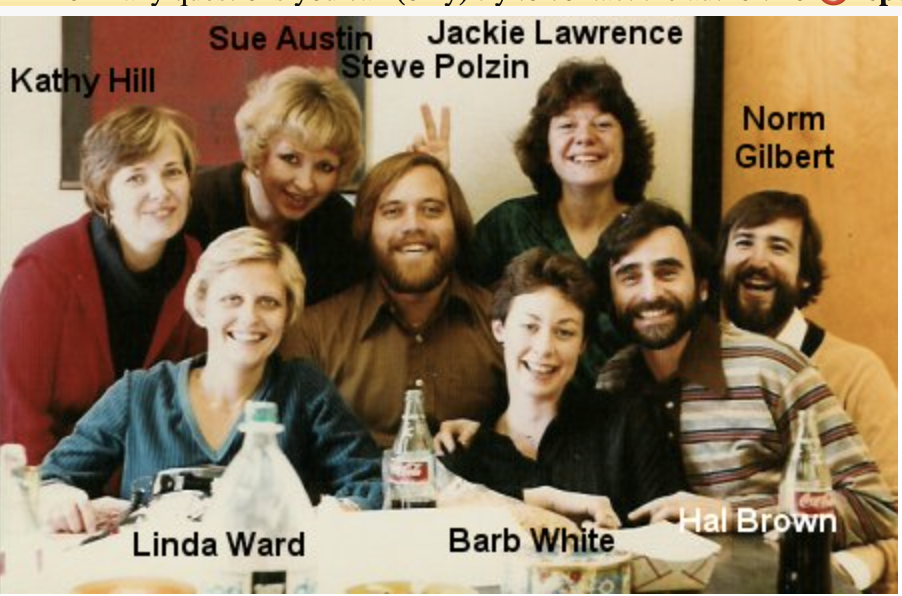
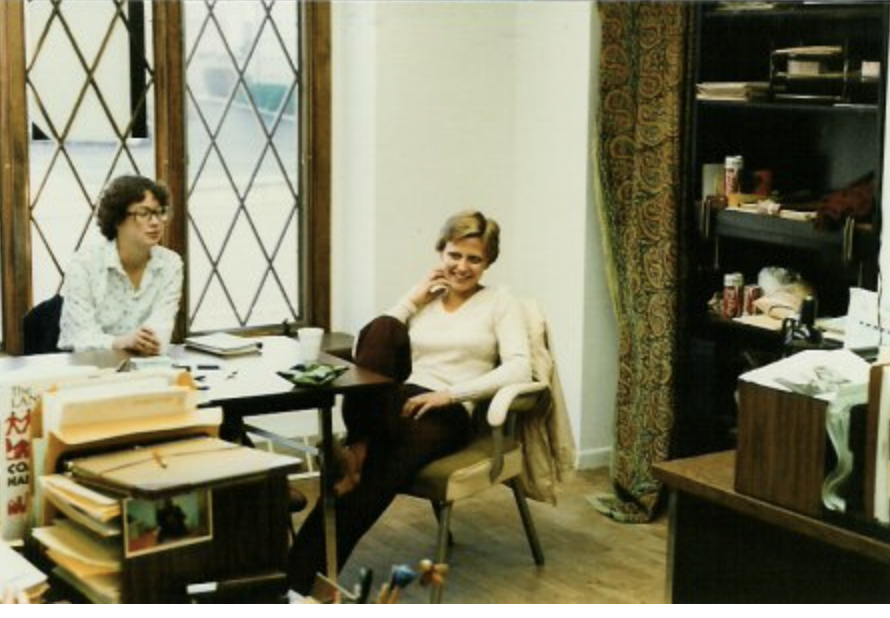
Why are these Mason Mental Health staff members smiling?
While our work was serious we always found time to relax among ourselves.

Click to enlarge (that's me in the striped shirt)

During the heyday of publicly funded mental health our program continued to grow. The staff increased and we moved our building to one with twice the space, and then increased our space there two-fold. We were able to provide service on a sliding fee scale and generally could see clients for as long as they needed therapy. Our paperwork requirements were minimal, and there was no such thing as managed care.

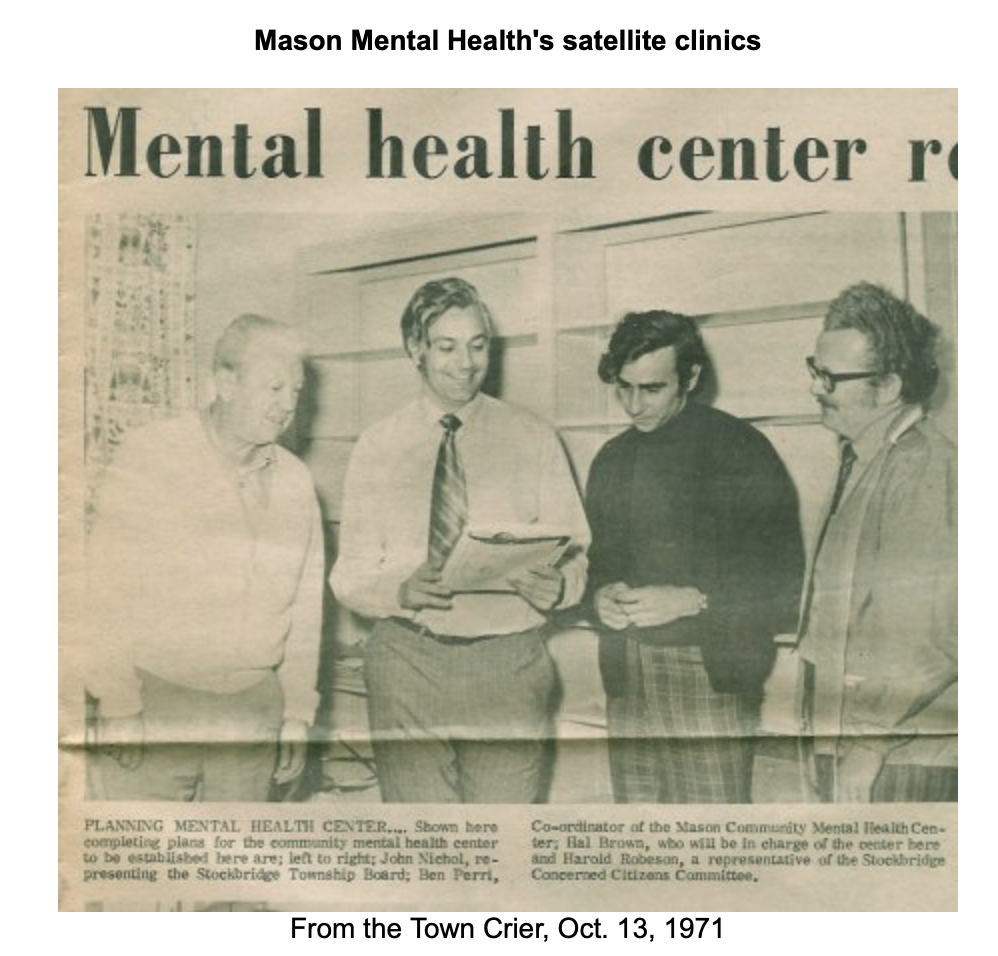
We called these one-day-a-week clinics satellites, and operated three of them.
Mine was in Stockbridge, Mel Scherpinesse ran one in Williamston, and Mary Louis
was in a tiny town called Leslie. These clinics were the first to close as budgets
were cut in the mid-1980's.
Fashion Comment: I'm glad I wasn't the only one wearing plaid pants in this photo.

From 1971 to the day it closed in 1989, Mason Mental Health increased its
physical size. In the building above, located in downtown Mason, we added
a day treatment program and doubled our size. Then after there was a "sick|
building" scare, when about half the staff began to suffer eye irritations, we were
forced to move to a large building (below) on the outskirts of town.

We began by occupying half of the new building, but eventually took over the other half.
The day there was a meeting where my bosses decided to close the center, we actually
had a carpenter converting a small office to a file room.
Read about our dubious distinction (click to enlarge):

We were one of the first offices to herald the epidemic of so-called "sick buildings." While I never got any symptoms, I observed both staff members and visitors have their eyes turn red and swell nearly shut after a short time in the building. Thousands of dollars were spent to see if there were any toxins or irritants present. Specialists were brought in from the state health department, Michigan State University and from two private firms. The Center for Disease Control even reviewed all the findings. All that was ever found was a minute amount of formaldehyde in the air, less than would be expected from any building where people smoked cigarettes.
Regardless of these scientific findings, we were forced to move to the temporary quarters in an old house, pictured below. The new tenants of the building never had any health problems.



Interestingly, we suffered no drop-off in client referrals while we occupied this building.
The rooms upstairs had no doors when we moved in, so we constructed and installed plywood doors ourselves. Day Treatment moved to the basement of the Farm Bureau two blocks away. For privacy we always had the radio blasting. Office space in the area was scarce, so for three months we had no idea when (or if) we would move. Despite the fact that we were working under trying conditions, we always found time
for a break.

In 1982, the Mason Mental Health Center was one of the first programs to receive a grant from the Veterans Administration to operate a program to treat Vietnam veterans suffering from delayed post traumatic stress disorder. In fact, I believe we were one of only two community mental health centers to receive such a grant. Eventually the VA itself opened outreach programs themselves all over the country, and programs like ours were phased out.
Our program began in November of 1981 without any involvement with the VA. Not a veteran myself, I had been working with a few Vietnam combat veterans in therapy. They were involved in a Vietnam veterans' organization and were contacted by the local PBS television station, WKAR in East Lansing, MI, to put together a group to take phone calls at the station after they aired a special on post Vietnam stress syndrome.
They suggested that I be one of the resource people available, not to take calls, but to assist those vets who were. The phone calls began to pour in after the program and I decided on the spot to offer a group at Mason Mental Health for any vets who wanted to attend. A few nights later 25 showed up for the first of many vets groups, and spin-off groups for spouses of vets.
That was how we did business in those days. If we saw a need, we tried to met it. We weren't volunteers, one of "the thousand points of light." We were paid for what we did, but we did it because it needed to be done. The real heroes of the Vietnam veterans programs were the clients themselves. They hung together and helped each other through touch times as they dealt with inner demons.
One man in particular went on to be appointed to the Governor's Agent Orange Commission where he distinguished himself, until he succumbed to a cancer that was probably caused by agent orange. I am certain he would give me permission to publish his name as he made no secret of having been part of the Mason Mental Health program as a client. I still have to maintain his confidentiality, but those who read this will know who he is.
I would have liked to keep the program independent from the VA, but I knew that I needed to hire a Vietnam veteran who was also a professional psychotherapist, and there weren't many of them around. So when VA funds became available I wrote the grant and we were able to hire the first of several dedicated therapists.
Unfortunately, the VA took over much of the control of the program and while it continued almost until Mason Mental Health closed, our relationship with the VA was never very good. They insisted on approving clients before we saw them, even for first time emergency sessions that we were willing to do for free. We had to attend regular meetings at a VA center 60 miles away, and our therapists ended up having two supervisors. One hated bureaucracies and the other seemed to thrive in one of the biggest bureaucracies in the government. One knew his therapists could empathize with Vietnam veterans far better than he could and the other... well, I'm sure you get the idea.

Mason Mental Health's Day Treatment program, as befitting a rural program,
had a large vegetable garden. They not only sold fresh produce to local supermarkets;
but donated vegetable to the local food bank.
The staff pictured are Steve Polzin holding a watermelon, Barb White in the
lavender blouse, and coordinator Linda Ward, seated in front. To protect
confidentiality, client's faces have been covered with cutouts from a magazine.

State State Representative Debbie Stabenow was a big supporter of the program. She is now a United State Senator from Michigan and has just announced she will retire at the end of her current term.
Mason Mental Health had day treatment program began as an experiment, which ultimately failed, and which developed into a model treatment program under Linda Ward who was hired in 1979. The earlier program included intensive group therapy which was central to its experimental component. Unfortunately this did not succeed. It was run by Michael Teixeira, then a doctoral student in clinical psychology at Michigan State University. He attempted to apply the theories of the late Michigan State University psychology professor Bertram Karon who was a proponent of a very active form of treating schizophrenia using psychoanalytic principles to our chronic clients.
In my own limited experience I had dramatic success applying these methods in my treatment with two clients who I thought were schizophrenic as they had carried that diagnosis for many years and through frequent psychiatric hospitalizations.
I believed we could do the same thing with our own day treatment clients, most of whom were diagnosed with schizophrenia. Over time, I saw little positive change in the day treatment clients and then realized that the clients I succeeded with had been misdiagnosed as schizophrenic, and their apparent delusions and hallucinations were really manifestations of dissociation caused by childhood trauma. Therefore I changed the methodology of the program and hired new staff.
Linda Ward came on board and developed a humanistic program where the emphasis was on relating to the clients with empathy and warmth, while working with them to establish mutually acceptable and realistic goals. Staff were always willing to reach out to clients during times of crisis and physically go to where the clients needed them to be, whether it be a group home or the public library where one of them might be having a panic attack.
Because the town of Mason was uniquely accepting of our clients, many of whom lived in group homes there, a hallmark of the program was its success in involving our clients in community life. Jackie Lawrence deserves much of the credit for this. She began working for the program as a secretary, but before long it became obvious that the clients were drawn to her and vice versa. She had an extraordinary knack for outreach, politics, and community relations. As soon as we had a vacancy, I hired her as a mental health worker and she has been an energetic anchor for the rural aftercare program in Ingham County ever since.

By the end of 1988, the fate of the Mason Mental Health Center, was all but sealed as the
tri-county program faced a $1 million budget cut for the coming year. In 1989 it was closed.
When Mason Mental Health Center was closed in 1989, it was replaced with the smaller Mason Rural Outreach Program (or Mason ROP) with Linda Ward as its coordinator. Along with Jackie Lawrence, Nancy MacKenzie and Lois Duling, the program moved into the downstairs of a small, rundown, house across an alley from the business section of Mason. The Mason ROP has earned accolades as one of the most innovative programs in the state of Michigan, but that is another story.
While the aftercare population of the rural part of the county receives excellent care, public comprehensive mental health service became a thing of the past when the Mason Mental Health Center was closed. All of its outpatient clients with the exception of a few children, who were still served by a part-time therapist, had to drive into Lansing for service.
I transferred to be the director of a similar program in one of the other three counties that made up the tri-county mental health program. This county was the same size as the area that the Mason Mental Health Center served, but the program there and in the second of the three counties, survive to this day because each is in a different county than Lansing.
I later learned that Mason Mental Health Center was sacrificed in order to save a few jobs at the main outpatient clinic in Lansing.
Staff
Mason Mental Health Center, Mason, Michigan
1971 - 1989
Supervisors
Ben Perri, PhD
Tom Helma, MA
Hal Brown, MSW
Support Staff
Joy Beights
Lois Duling
Jean Emerick
E. Fuller
Kathy Hill
Barbara Hollenbach
Ellen Martinson
Pat Oakes
Sue Stone
Treatment Staff
Susan Austin, MSW
Jane Bell, OTR
Marilyn Braman
Shirley Brown, MA
Cindy Carlson, MSW
Maureen Chaisson, MSN
Keith Dedrich, MSW
Patricia Foreman, MEd
David Fugate, MA
Clark Etterman, MSW
Normand Gilbert, MA
Gail Gingrich, MSW
Molly Gee, MSN
Claudia Gostine, BS
Donald Healey, MA
Beverlee Kagan1, MSW
Barbara Katz, MSW
Jackie Lawrence
Mary Louis, MSW
Nancy MacKenzie, BRT
James Meuller, BA
Joan Penfield, BSW
Michael Pierce, MSW
Steve Polzin, MSW
Toby Powell, MSW
Gwen Reid, BA
Mel Scherpenisse, MA, PhD (died Mar. 24, 2022)
Rikki Schoenthal, MSW
Nancy Spaninga, BA
Michael Teixeira, MA
Barbara Thiebeau, MSW
Becky Thompson, MSW
Linda Ward, BSW
Toni Warley-Mansion, MSW
Penny Wepfer, BA
Barbara White, MSW
Margo Winkler, MSW
Jean Zugger, MSW
(many of the above staff have since earned higher degrees)
Medical Staff
Luther Goldschmidt, MD
Malcolm Johnston, DO
Alex Lebedovych, MD
Gerald Osborne, DO
Footnotes:
1. Beverlee Kagan passed away in Florida in 2002
This is a list compiled from memory. If I left someone off, or spelled a name wrong, I'm sorry.
I'm always interested in hearing from former staff as well. In fact, I just ran into a Mason Mental Health Center therapist who I hadn't seen in over twenty years at a seminar. With 1,000 attendees, he ended up sitting directly behind me in the first workshop. Neither of us knew we were both living in Massachusetts.
It was my chance encounter, and delightful reminiscing, with him that led me to dig up these old photographs and put together this brief illustrated history of Mason Mental Health.
More about me:
In addition to practicing psychotherapy, I was the supervisor of two rural mental health centers, a clinical supervisor, and a field instructor helping to train clinical social workers from both Michigan State University and the University of Michigan. I've presented workshops at several state and two national conferences on a variety of clinical topics. I also particpated in research conducted by Dr. Norman Kagan in a training method called Interpersonal Process Recall (IPR) and made several training films with a real client.

Due to budget cuts the Mason Mental Health Center was closed and I was moved to a sister satellite center in St. Johns, the Clinton County Counseling Center. This entailed driving nearly an hour to get to work, quite a change when my office was five minutes from home.
This was after I discovered that the program was held in lower regard by the heads of the other agencies in the county than I had been told.
The steps I took unilaterally without clearing them with my superiors led to a temporary suspension, which I fought with a lawyer and eventually won a pyrrhic victory and was returned to run the program under untenable circumstances. It was so bad I wasn't allow to work in my office even doing clinical supervision with staff with the door closed. If was seeing a client I could have closed the door of course but the entire time I was there the admissions staff refused to refer clients too me.
Here's how the Lansing paper described what happened at the Clinton County Counseling Center.
 |
All the heads of the country agencies wrote me glowing recommendations when I left.

I was in general adult practice where I worked with patients who were businessmen and women, construction and trade workers, housewives, professors, college students, farmers, techies in the electronics and computer industry and executives.

I also have had considerable experience working with with police officers and correction officers in both individual and couple's therapy.
Because I spent 20 years as an auxiliary police officer in two cities I learned about police stress, I published the number one website on the subject, Police Stressline. I began the website by posting articles I originally wrote for a print Massachusetts police magaize called Police Log. Some of the online articles were picked up and published in print police magazines. Read Daily Kos article about my police experience.


My Massachsetts office was very private. It was at home with its own waiting room and entrance, overlooking the cranberry bogs which, until the summer of 2006 when they were sold, were owned by my wife and her family.
My late wife Betty and I were Ocean Spray grower-owners and we published one of the first websites to have a major impact on an entire industry, Cranberry Stressline. Because it brought together growers from across the country when there were problems with the management of Ocean Spray the website was credited with promoting a proxy war which resulted in the election of a new board of directors and the firing of the CEO, Robert Hawthorne.
As a therapist I worked with people with anxiety, depression and relationship problems, with people who are compulsive, irritable, anxious, and those who suffer from self-doubt and self-esteem problems. I also worked with people who were struggling with more existential questions such as who they are and what their life was all about.
I always believed therapy should be a partnership between client and therapist, and that the basis for good therapy is trust, and that it was my responsibility for seeing to it that clients weren't spinning their wheels fruitlessly while I sat back and wait for them "to get it on their own," while I had a pretty good idea where they had to go to resolve their problems.
My understanding of personality dynamics comes from being trained in psychodynamic and psychoanalytically oriented therapy in the master's program at Michigan State University in the early 1970's. While I did not have post-graduate training in this area (I am not a psychoanalyst), I had considerable experience in providing therapy that was aimed at helping clients gain insight into themselves and how their family of origin influenced who they are.I didn't have any particular "brand" of psychotherapy that I practiced, especially since the type of therapy I provided depended on the client's needs and desires. Generally for symptom reduction alone, therapy that gives a client support and encouragement, and helps them better understand self-defeating behaviors and change them, is the most effective.
I also blended what is known as cognitive-behavior therapy into my approach as needed. Basically this helped the client to recognize and change their self-defeating thoughts and behaviors. Whether focused on behavioral change or not my approach to my clients was always informed by my understanding of psychodynamics.
I have discovered over many years that it's the personality of the therapist, their ability to listen, and the connection he or she makes with the client that dictates success or failure in therapy. I tend to be suspicious of any of the "therapy of the month" flavors of treatment often touted in best selling books and by their authors on talk shows.
My own understanding of the incredible power of the mind to protect a person from the memories of abuse, especially prolonged childhood sexual abuse, came working intensively with a number of clients who I was the first clinician to recognize were suffering from what was at the time called multiple personality disorders(now called dissociative identity disorder). The hallmark sign of this disorder is that the person experiences amnesia for significant persons of time. This occurs when another personality, or alter, is in control. This would be the subject of another article.
Other online activities:
I was a weekly columnist for the website Capital Hill Blue for several years. I also had an online column called The Eclectic Digest which was publshed in two large daily papers south of Boston, The Brockton Enterprise and The Patriot Ledger.


Here's a blog about my late wife Betty and my life growing cranberries.
New: My essays from when I wrote a weekly politcal column for Capitol Hill Blue circa 2009. || Archive of Daily Kos articles ||
.